Comparative Analysis of Preclinical Dental Students’ Working Postures Using Dental Loupes and Dental Operating Microscope
Marius Bud, Razvan Pricope, Razvan C Pop, Razvan Onaca, Pieter-Jan Swerts, Ondine Lucaciu, Ada Delean
ABSTRACT
Background: Dentists are susceptible to musculoskeletal disorders due to prolonged static postures during dental treatments. Using a magnification tool like dental operating microscope (DOM) or the dental loupes, may correct the operator’s posture. Up until now few studies have focused on preclinical dental students’ posture when working with the DOM, while most of them have focused on the loupes. The aim of this study was to comparatively analyse the working posture of preclinical students during a dental restoration procedure, working with two different magnification methods.
Materials and methods: This study used a randomised cross-over design in which seventeen third year students were randomly divided into three groups. The exclusion criteria were previous contact with magnification systems and previous clinical working experience. Each student prepared 3 Black class 1 cavities on artificial lower molars: first with no magnification, following dental loupes and DOM. They were video-recorded throughout the preparation. Trunk, neck and upper-arm position was evaluated using the Posture Assessment Instrument. Students completed a questionnaire on their subjective perception of the two magnification systems.
Results: The statistical analysis showed significant improvement of the working posture using magnification systems compared to direct vision. The biggest improvement was obtained through the use of DOM, followed by the dental loupes. Students perceived dental loupes as being the most comfortable and easy to adapt to. They reported being more focused when using DOM.
Conclusions: Both magnification systems had a positive impact on the working posture, DOM having the best results. Loupes showed better adaptability while DOM showed better concentration.
Key words: posture, microscope, loupes, magnification, student, restorative dentistry
INTRODUCTION
Musculoskeletal disorders (MSD) are described as disorders of the muscles, tendons, ligaments, joints, cartilages, intervertebral discs or nerves,1 most often represented by inflammatory disorders as bursitis, synovitis, tendonitis and tenosynovitis as well as degenerative osteoarthritis.2,3,4 The MSDs that affect most dentists are located in the trunk, neck and shoulders.5,6,7 By affecting the bones, muscles and joints ,8 the most frequent manifestations are pain, muscular imbalance, paralysis or muscular dysfunction.9 These have the potential to affect the quality of life and work schedule, increasing the frequency of absenteeism from the workplace, and can sometimes lead to injuries that can cause put a premature end to the professional’s career.10-13
Dentistry belongs to a category of professions that have a higher predisposition towards developing musculoskeletal disorders (MSDs) because most dentists cannot avoid extended static positions. Even with optimal posture, more than half of the body muscles are contracted statically.14 Thus, due to repetitive unnatural movements and the inadequate equipment or inadequate design of the dental office, dentists belong to a category that has an increased risk for developing MSDs.5,6,9
Although the subject of ergonomics is widely discussed and ergonomics is taught in most dental schools , some practitioners may skip applying ergonomic principles due to lack of theoretical knowledge or the inability to put them into practice.15Furthermore, inexperienced dental students, focusing more on improving their visual examination skills, hand-eye coordination and spatial awareness are more likely to overlook ergonomics, which places them at risk of developing poor working postures in the future. Trying to combat these affections, the science of ergonomics searched for multiple methods to improve. Among those methods, magnification systems proved to be an efficient tool to combat ill posture and subsequently MSDs.16Magnification loupes, shown to have positive impact on the prevention of MSDs,16 could improve students’ working habits because students who have begun their clinical years are more prone to work-related musculoskeletal disorders compared to students in their preclinical years. 17
Studies have indicated a reduction of the incidence and severity of MSDs in dentists by the proper use of magnification systems because it ensures the optimum visibility of the operating field when maintaining an ergonomic position.13,18 The use of magnifying loupes in dentistry showed an improvement in the doctors’ working posture, with a decrease in the severity and symptomatology of MSDs, in particular by reducing the craniovertebral angle.18,19
Of the magnification systems, the microscope offers the highest magnification degree and the most neutral working posture.19 Yet, there is little to no literature available about the dental microscope as a means to improve working posture, moreover there is even less literature comparing the ergonomic benefits brought by the loupes to those brought by the microscope.
Branson’s modified posture assessment index20 can be used to quantify the changes in body position and compare them to the ideal body posture. Our study aimed at assessing whether different magnification systems could positively influence preclinical students’ working posture, and if so, which of the magnification systems brought the biggest improvement. We also wanted to evaluate the students’ subjective perception of the magnification systems with the help of a questionnaire.
MATERIALS AND METHODS
For this study we used a randomised crossover design. Eighty students in their third academic year were invited for this study, from which only seventeen were selected after applying the inclusion criteria: having no previous clinical working experience and having successfully passed their Ergonomics and Cariology exams. Therefore, all students who participated in the study had knowledge of cavity preparation and ergonomics acquired in lectures and preclinical trainings from previous academic years. The sample of dentistry students formed its own control group. Each student was provided with a workstation consisting of a dental simulator unit (Zhengzhou Linker Medical Equipment Co., Ltd., China) with a high speed handpiece (NSK Company, Japan) with water spray coolant, dental loupes (Orascoptic HDL, Madison, USA, 2.5x magnification, Endeavor lighting), dental operating microscope (OMS 2350, Zumax Company, China, 1.6x magnification and 20W LED coaxial illumination ), a dentist stool, an examination kit, a high speed straight cylinder diamond bur (Kerr Company, Germany), and a periodontal probe for measuring.
Each student’s task was to prepare a Black class I cavity with a depth of 2.5 mm and a minimum diameter of 2 mm on the first mandibular molar on the right side, mounted on the dental arch of the simulator. The students prepared the cavities using each of the 3 methods presented for comparison: the unaided eye, dental loupes and dental microscope. Before starting the actual task, they received a minimal training regarding the optical adjustment of the microscope and loupes in which they were instructed on how to make the optical adjustments on both DOM and the loupes. After adjusting the devices, each device was checked by a medical doctor with more than 5 years’ experience in using the microscope and dental magnifying loupes. Each student has individually determined his ergonomic working position. The participants were randomly separated into three groups , first two groups with six students and the third with only five. Group 1 started their first working session, which involved preparing the cavity in unaided vision conditions for a total time of 10 minutes. Upon finishing, they received a 10 minute break, in order to eliminate fatigue as a limiting factor, and also during which the artificial tooth was replaced. Group 1 started their second working session involving preparation with the aid of magnifying loupes for another 10 minutes followed by another 10 minute break. The group finished with their third working session under the magnification of the microscope. Group 2 and 3 followed in the same manner. Therefore, by the end of the experiment, each student had prepared three separate cavities, one using each of the three compared methods, starting with the unaided eye and finishing with the microscope.
All students were video recorded throughout the preparation of their three cavities with the help of two video cameras, one placed in the back and one to the side of the operator. Three independent observers followed all the recordings and analysed the position of the subjects in terms of the number of unnecessary movements they made while working, the position of the trunk, head and neck, and shoulders. The observations were quantified using Branson’s modified PAI (Posture Assessment Instrument), analysing the number of movements, and offering a score from 1 to 3 points for the trunk and head-neck, and from 1 to 2 points respectively for shoulder posture. Each position maintained for more than 10 seconds was evaluated and graded. The score of 1 represented the best value and implicitly the closest position to the ideal whereas 3 points were given where a body segment had an angulation of more than 45 degrees from the ideal. Upon finishing a preparation, each student received a final score for every criterion evaluated (trunk, head-neck and shoulders). The final score represented the average of the points awarded during the 10 minutes of cavity preparation. Thus, lower PAI scores indicate a working posture that is closer to the ideal. Also, for a global view of the posture adopted by each student, we calculated a global PAI score, representing the average of all the final scores for each student.
The results were analysed using the paired Student test, comparing the number of movements, as well as the PAI scores of each magnification system and the unaided eye, and between the two magnification systems themselves. Upon completion of the three working sessions, the students answered a Likert 1 to 5 scale where 5 was the highest possible score (i.e. 1=very uncomfortable; 5=very comfortable) questionnaire evaluating : their subjective perception regarding the comfort of their working position, ease of adaptation, impact on their posture, concentration during work and fatigue at the end of the work sessions depending on the magnification system used. They were also asked to pick their preferred system for future use. The results of the questionnaire were analysed so as to provide a comparison between the 3 vision methods for each criterion evaluated, using the Student test for unpaired samples.
RESULTS
The primary aim of this study was to assess whether different magnification systems could improve dental students’ working posture while the secondary aim was to determine which magnification system brought the biggest improvement in the working posture.
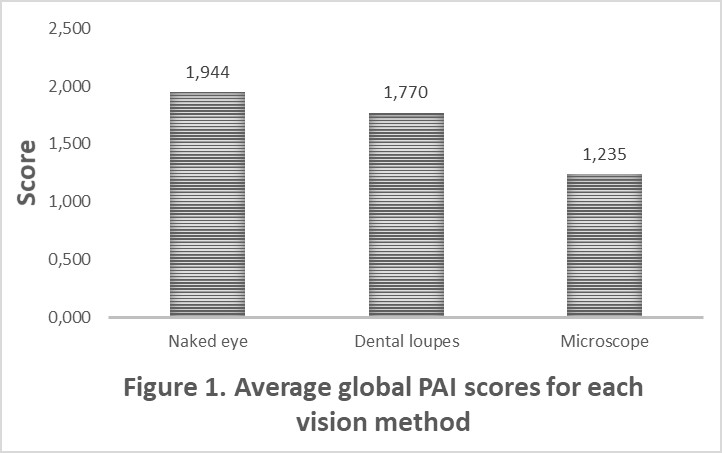
Regarding the global PAI score, (Table 1) the mean differences were 0.17 between the unaided eye and dental loupes (p = 0.0041), 0.70 between the unaided eye and the DOM (p <0.0001), and 0.52 between the dental loupes and the DOM (p <0.0001). The average global PAI score for each vision method is ranging between 1.235 and 1.944 (Figure 1).
The mean difference in the number of movements (Table 1) between the unaided eye and magnifying loupes was 3.06, which is not statistically significant (p = 0.0775). However, when it came to comparing the unaided eye to DOM and dental loupes to the DOM, the results were statistically significant: – 9.35 (p = 0.0002) and – 6.29 (p = 0.0050), respectively.
All the mean differences between the scores obtained during working with the unaided eye, dental loupes and dental operating microscope (DOM) (Table 2) samples were statistically significant, for all three body segments analysed (trunk, head and neck, shoulders).
When analysing the head-neck segment (Table 2) the mean difference between the unaided eye and dental loupes was 0.27, (p = 0.0012), 1.1371 between the unaided eye and the DOM (p <0.0001), and 0.86 between the dental loupes and the DOM (p <0.0001).
For the trunk segment, (Table 2) the mean difference between the unaided eye and dental loupes was 0.14 (p = 0.027), 0.55 between the unaided eye and DOM (p <0.0001), and 0.40 between dental loupes and the DOM (p <0.0001).
For shoulder posture, (Table 2) the mean difference between the unaided eye and dental loupes was 0.11 , (p = 0.0413), 0.43 between the unaided eye and the DOM (p <0.0001), and 0.32 between the dental loupes and the DOM (p <0.0001).
We also wanted to determine each students’ subjective perception about the magnification systems through a questionnaire. We assessed the degree of comfort reported by students during the task, their subjective perception on the correctness of their posture during the working sessions, the fatigue they perceived after finishing each task and the level of perceived attentiveness while working. Students were also asked to evaluate the ease of adaptation to the working posture for each magnification system and to indicate which magnification system, if any, they preferred for their future practice. The average scores for the aforementioned categories can be seen in Figure 2.
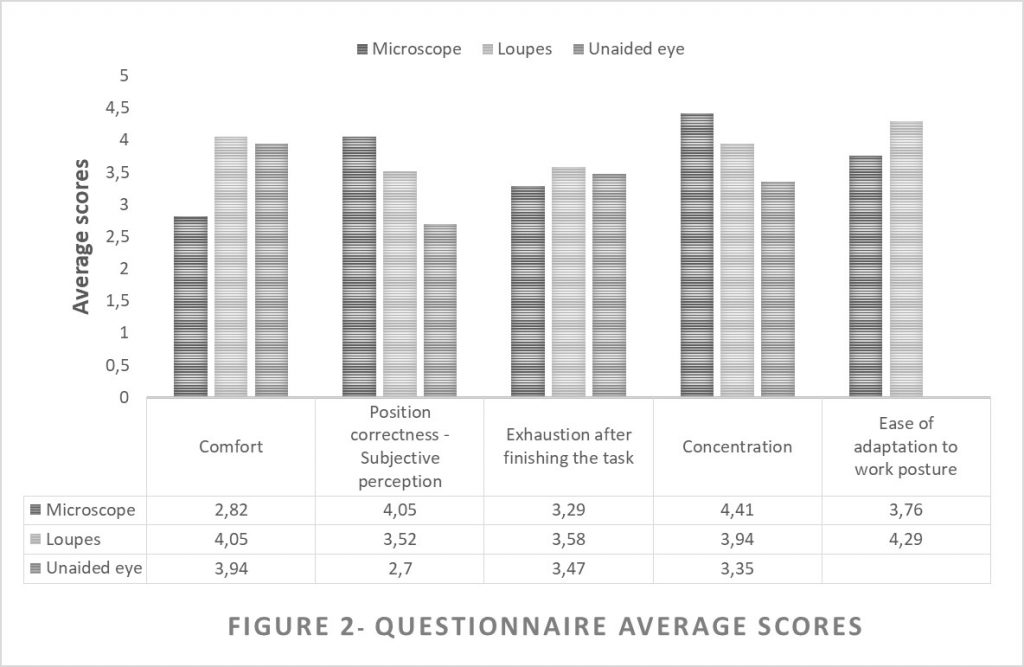
The average scores for the comfort students reported during the tasks were 3.94 for the unaided eye, 4.05 for the dental loupes, while for the microscope it was 2.82.
The subjective perception on the correctness of the posture adopted during the tasks had the following average scores: 2.7 for the unaided eye, 3.52 for the loupes and 4.05 for the microscope.
For the fatigue perceived by students after finishing each task, the answers varied from 1 to 5 but the average score reported was 3.47 for the unaided eye, 3.58 for the loupes and 3.29 for the microscope.
The answers ranged from 2 to 5 for the level of perceived attentivenessduring the task, with the average score for the unaided eye being 3.35. The average score for the loupes was 3.94, while for the microscope it was 4.41.
The average scores for the ease of adaptation to the work posture for each magnification system were 4.29 for the loupes, while for the microscope it was 3.76.
Regarding which vision method students preferred for their future practice, all of the students wanted to use a magnification system in their future practice. The loupes were preferred by 64.7% of the students, while the other 35.3% chose the microscope.
Upon statistical analysis, the comfort difference between the unaided eye and the loupes was found to be statistically insignificant (p=0.71). However, when it came to comparing the unaided eye against the DOM, the average difference in score was 1.12 points (p=0.0002), while for the dental loupes versus the DOM, the average difference in score was 1.24 points (p=0.0001).
Regarding the subjective perception on the correctness of the posture adopted during the tasks, the average difference in score between the unaided eye and the loupes was 0.82 (p=0.0017), while that between the unaided eye and the microscope was 1.35 (p=0.0001). Between the loupes and the microscope, the average difference in score was 0.53 (p=0.0221)
When analysing the fatigue perceived by students after finishing each task, all the differences in scores were statistically insignificant, with p taking values of 0.772, 0.6555 and 0.5275 respectively.
The level of perceived attentiveness during the task was not statistically significant between the average scores of loupes and microscope (p=0.0694). Statistically significant differences in average scores were found between the unaided eye and the loupes (0.59; with p=0.0107) and between the unaided eye and the microscope (1.06; with p=0.0001).
The difference in average scores of the loupes and the microscope regarding the ease of adaptation to work posture was statistically insignificant (p=0.0878).
DISCUSSIONS
For this study we analysed the working postures of seventeen dental students with no previous clinical experience during the preparation of Black class I cavities using as vision techniques the unaided eye, dental loupes and DOM. Based on our results, both the loupes and the microscope improved the overall posture of the students when compared to the unaided eye vision technique, confirming our expectations.
The use of the DOM improved the overall posture of the students by 36%, with an average PAI Score difference of 0.70 points (p<0.0001) when compared to the unaided eye vision technique. The use of loupes also confirmed out expectations and improved the overall posture of the students by 8.9%, (p=0.0041), as shown by Carpentier et al. 21
Regarding the subjective perception on the correctness of the posture adopted during the tasks, students confirmed our results, unaided eye vision being rated with the lowest average score of 2.7 points, dental loupes with 3.52 points, and the microscope scoring highest with 4.05 points out of 5.
These results are indicating a clear distinction between magnification systems and simple, unaided vision, when comparing ergonomic scores. The dental microscope not only provides better magnification of the working field, but also forces the practitioner to sustain an ergonomic, straight back position throughout working sessions. On the other hand, the learning period when working with the microscope is quite long and the use of a microscope may significantly increase the time needed to complete a treatment among practitioners with less than three years of microscope work experience.22 Despite all that, studies indicate a high degree of student compliance with using magnification and an enhancement in student performance during preclinical dental practice.23
Even though dental students possess good theoretical knowledge of dental ergonomics, their clinical practice may be affected by the lack of training and experience. Working with high speed rotary instruments needed to prepare cavities, students require good hand precision and good eyesight in order to obtain successful treatments and to avoid dental iatrogenesis. Therefore, they are often tempted to pay less attention to ergonomics. This behavior may lead to back pain or hand and wrist problems, as more stress is placed on the spinal disks when lifting, lowering, or handling objects. Using dental loupes or dental microscope may improve the working posture due to the reduced working distance, higher magnification and better lighting.24
Even if students are less likely to use magnification in most dental schools, our research, supported by previously published literature, is showing a significant improvement in students’ posture when working with magnification. Peggy at all. (2008) showed a significant postural benefit in using dental loupes immediately after entering the program compared to students who delayed that until the second semester.25
Based on our results, both the loupes and the microscope had a positive impact on the posture of dental operators. When comparing microscope vision with loupes vision, we found that the microscope leads to a significant posture improvement of 30.2% (p<0.0001 with 95% C.I.) compared to the dental loupes. Therefore, we should take into consideration the introduction of magnification systems in restorative treatment working protocols for the university students in order to improve their posture. Moreover, the questionnaire showed that students feel more confident when working with magnification and they believe that using magnification may be mandatory for their clinical work in the future, as further suggested by other studies.26
A big improvement in the posture of the trunk was noticed when using loupes and microscope (an improvement of 8.2%, and 32.6%, respectively). This can be explained by the fact that, more often than not, when not using a magnification system there is a tendency to bend over the patient to get the eyes closer to the patient’s mouth, so as to obtain a good view of the oral cavity, and that inevitably involves bending the spine. Additionally, the patient sitting in the dental chair is lower than the dental practitioner’s field of view, therefore inexperienced practitioners feel the need to bend their head and neck forward. We found significant differences between trunk posture when working with loupes and with a microscope, the latter showing a 26.4% improvement in back posture (p<0.0001), which confirmed our initial expectations: the microscope is far superior in ensuring a proper trunk posture during working sessions.
The use of a microscope showed an improvement of 50%, (p<0.0001) in head and neck posture and 23.6% in the posture of the shoulders. These results indicate a major role of the dental microscope in overall dental ergonomics.
When loupes vision was analyzed, the overall ergonomic improvement was around 4 times less than microscope vision: 11.89%, improvement (p=0.0012) in head/neck posture and 5.9% (p=0.0413 ) in the shoulder posture.
Shanalec27 and Juggins 28 reported that the use of loupes requires a minimal work distance between the dentist’s eyes and patient’s oral cavity, which is compatible with the neutral posture of the spine and neck, avoiding musculoskeletal disorders.14,29 Additionally, other advantages such as increased comfort and lower incidence of pain, especially in the spinal region, are observed.30,31
Overall, the microscope vision allowed students to obtain better posture ergonomics. No significant differences were found for the posture of the shoulders when it came to comparing work with a microscope and loupes versus work with the unaided eye (23.6% and 5.9%). This may be due to the fact that shoulders can still move freely, no matter the magnification system, unlike the trunk and the head/neck, which are on a “locked” position when working on a microscope. As a consequence, the movements of the head/neck and trunk are significantly reduced, in order for the operator to keep his field of vision through the eyepieces.
Students with high number of movements while working are more prone to fatigue and unnecessary muscle contraction. Our data shows a significant drop of 60.6% (p=0.0002) in the number of movements of the dental operators when a microscope was used.
The loupes offer magnification but still permit the body to move, affecting the ideal ergonomics. Even so, there was a 19.8% reduction in the number of movements when dental loupes were used versus when working with the unaided eye (p=0.0775 with 95% C.I.). Thus, we may conclude that magnifying the image of the working field decreases the number of operator movements. In any case, when asked to choose the vision method preferred for future dental practice no student chose the unaided eye. Since all the students preferred using a magnification system, when given a choice between loupes and microscope the former were preferred by 64.7% of the students, while the latter were preferred by 35.3%, who wanted to use the microscope in the future practice. We consider our results to be of clinical relevance because the students have reported higher comfort using the magnification systems and better concentration.
Given the increased adaptability of the loupes, they could be a first step for medical students and young dentists in using magnification, before moving on to the microscope. Although loupes offer unique magnification, it is lower than that provided by the clinical microscope, which is why their use may be related to cervical injury.27 Furthermore, Zaugg et al. [2004] reported that using a microscope resulted in fewer errors than when a set of loupes was used.32
Given the positive feedback received after working with the magnification systems, an important step in the development of dental education and the prevention of MSDs would be implementing them in student work placements, thus allowing students to become familiar with them from the first clinical years. Although it is the hardest to adapt to, we recommend the use of the microscope in daily practice due to the significant positive influence on MSDs. To begin with, we recommend the magnifying loupes, since they provide a much more manageable learning curve.
A possible limitation of our study can be our relatively small sample size. A larger sample size of students would have given a more broad statistical analysis , although the differences between students’ scores were quite high. Another limitation can be that we used a modified PAI. Using the complete PAI would have resulted in a more complete set of data about the influence of magnification systems on students’ working posture. Also, the students in our sample only worked on the first mandibular molar, which doesn’t force the student to work in a very unnatural position. Future research can be aimed at using a different tooth or a different method of preparation such as for crown or inlays.
CONCLUSIONS
Both magnification systems had a positive impact on the students’ working postures, with the best results observed when working with the help of the microscope. The students reported that the dental loupes showed better adaptability and the microscope conferred a higher degree of attentiveness while working. Although they are expensive and the time for adjustment is longer, we recommend the loupes as a starting magnification system for students during restorative procedures, followed by the introduction of the microscope in the later years.
REFERENCES
- Kakosy T, Németh L. Musculoskeletal disorders caused by hand-arm vibration. Global Occup Health Network. 2003;4(winter):3–6.
- Carvalho MV, Cavalcanti FI, Miranda HF, Soriano EP. Partial rupture of supraspinous tendon in a dentist: A case report. FIEP Bull. 2006; 76:131.
- Doorn JW. Low back disability among self-employed dentists, veterinarians, physicians and physical therapists in The Netherlands. Acta Orthop Scand. 1995;263(Suppl):1–64.
- Suedbeck JR, Tolle SL, McCombs G, Walker ML, Russell DM. Effects of Instrument Handle Design on Dental Hygienists’ Forearm Muscle Activity During Scaling. J Dent Hyg. 2017;91(3):47-54.
- Gaowgzeh RA, Chevidikunnan MF, Al Saif A, El-Gendy S, Karrouf G, Senany S. Prevalence of and risk factors for low back pain among dentists. J Phys Ther Sci . 2015; 27(9): 2803–2806.
- Bernacki EJ, Guidera JA, Schaefer JA, et al.: An ergonomics program designed to reduce the incidence of upper extremity work related musculoskeletal disorders. J Occup Environ Med. 1999;41:1032–1041.
- Shaik AR, Rao SBH, Husain A, D’sa J. Work-related musculoskeletal disorders among dental surgeons: a pilot study. Contemp Clin Dent 2011;2(4):308-12.
- Movahhed T, Dehghani M, Argham, S, Arghami A. Do dental students have a neutral working posture? J Back Musculoskelet Rehabil. 2016; 29(4), 859–864.
- Yamalik N. Musculoskeletal disorders (MSDs) and dental practice Part 2. Risk factors for dentistry, magnitude of the problem, prevention, and dental ergonomics. Int Dent J. 2007;57(1):45–54.
- Morse T, Bruneau H, Dussetschleger J. Musculoskeletal disorders of the neck and shoulder in the dental professions. 2010; 35:419– 429. 411p
- Crawford L, Gutierrez G, Harber P. Work environment and occupational health of dental hygienists: a qualitative assessment. J Occup Environ Med. 2005; 47:623-632
- Brown J, Burke FJ, Macdonald EB, et al. Dental practitioners and ill health retirement: causes, outcomes and re-employment. Br Dent J. 2010;209: E7.
- Plessas A, Bernardes Delgado M. The role of ergonomic saddle seats and magnification loupes in the prevention of musculoskeletal disorders. A systematic review. Int J Dent Hyg. 2018;16(4):430–440.
- Valachi B, Valachi K. Mechanisms leading to musculoskeletal disorders in dentistry. J Am Dent Assoc. 2003; 134:1344–50.
- Pîrvu C, Pătraşcu I, Pîrvu D, Ionescu C. The dentist’s operating posture – ergonomic aspects. J Med Life. 2014;7(2):177-182.
- Lietz J, Ulusoy N, Nienhaus A. Prevention of Musculoskeletal Diseases and Pain among Dental Professionals through Ergonomic Interventions: A Systematic Literature Review. Int J Environ Res Public Health. 2020;17(10):3482.
- Khan SA, Yee Chew K. Effect of working characteristics and taught ergonomics on the prevalence of musculoskeletal disorders amongst dental students. BMC Musculoskelet Disord. 2013;14:118
- Valachi B, Valachi K. Preventing musculoskeletal disorders in clinical dentistry. J Am Dent Assoc. 2003;134(12):1604–1612.
- Hayes MJ, Osmotherly PG, Taylor JA, Smith DR, Ho A. The effect of loupes on neck pain and disability among dental hygienists. Work. 2016;53(4):755-762.
- Ng A, Hayes MJ, Polster A. Musculoskeletal Disorders and Working Posture among Dental and Oral Health Students. Healthcare (Basel). 2016;4(1):13.
- Carpentier M, Aubeux D, Armengol V, Pérez F, Prud’homme T, Gaudin A. The Effect of Magnification Loupes on Spontaneous Posture Change of Dental Students During Preclinical Restorative Training. J Dent Educ. 2019;83(4):407-415.
- Bowers DJ, Glickman GN, Solomon ES, He J. Magnification’s effect on endodontic fine motor skills. J Endod. 2010;36(7):1135–1138.
- Maggio MP, Villegas H, Blatz MB. The effect of magnification loupes on the performance of preclinical dental students. Quintessence Int. 2011 Jan;42(1):45-55.
- James T, Gilmour AS. Magnifying loupes in modern dental practice: an update. Dent Update. 2010;37(9):633-636.
- Maillet JP, Millar AM, Burke JM, Maillet MA, Maillet WA, Neish NR. Effect of magnification loupes on dental hygiene student posture. J Dent Educ. 2008;72(1):33-44
- Forgie AH. Magnification: what is available, and will it aid your clinical practice? Dent Update. 2001;28(3):125-130.
- Shanelec DA. Optical principles of loupes. J Calif Dent Assoc. 1992;20(11):25-32
- Juggins KJ. Current products and practice: The Bigger the Better: Can magnification aid orthodontic clinical practice? J. Orthod. 2006;33(1):62-66
- Congdon LM, Tolle SL, Darby M. Magnification loupes in U.S. entry-level dental hygiene programs-occupational health and safety. J Dent Hyg. 2012; 86(3):215-222
- Van As GA. Magnification alternatives: Seeing is believing, part 2. Dent Today 2014;32(8):80-4.
- Meraner M, Nase JB. Magnification in dental practice and education: Experience and attitudes of a dental school faculty. J Dent Educ. 2008;72(6):698-706.
- Zaugg B, Stassinakis A, Hotz P. Influence of Magnification Tools on the Recognition of Simulated Preparation and Filling Errors. Schweiz Monatsschr Zahnmed. 2004; 114(9):890–896.
Data Availiability Statement: The data that support the findings of this study are available from the corresponding author upon reasonable request.
Disclosure Statement: None of the authors have any conflict of interest to disclose. The companies that provided the loupes and the microscopes ( Orascoptic and Zumax) had no role in the design of the study or any interest in the reporting of the results.








